01. WHAT IS PATM
P.A.T.M. is a condition where individuals emit volatile organic compounds (VOCs) through their skin that trigger immediate, physical irritant responses in nearby people. The reactions are real -- sneezing, coughing, throat clearing, eye rubbing, nasal congestion -- typically within a 1-to-2 meter radius.
Sufferers experience profound social isolation and career disruption, yet exhibit no allergic symptoms themselves. The condition has no ICD code, no standard diagnostic protocol, and no approved treatment as of 2026. Most physicians dismiss it as psychosomatic.
KEY DISTINCTION
PATM is not about the patient smelling bad. It's about the patient emitting chemical irritants that provoke physical reactions in others. The patient often cannot smell anything themselves. This separates it entirely from standard body odor.
02. DIFFERENTIAL DIAGNOSIS
Before examining the evidence, PATM must be isolated from recognized conditions to prevent misdiagnosis. These are the most common incorrect theories applied to sufferers.
O.R.S. / SOMATIZATION
Olfactory Reference Syndrome & Somatic Symptoms
ORS is a psychiatric condition characterized by a preoccupation with emitting a foul body odor undetected by others. Mainstream medicine categorizes PATM under ORS or somatic symptom disorders, attributing bystander reactions (sneezing, coughing) to confirmation bias. However, research reveals a vicious cycle: initial low-level metabolic VOC emissions trigger mild bystander reactions, inducing acute patient anxiety; this sympathetic panic causes vasoconstriction, reducing hepatic perfusion and causing mitochondrial stress, which shuts down Cytochrome P450 enzymes and increases dermal VOC emissions.
T.M.A.U.
Trimethylaminuria
A genetic FMO3 enzyme deficiency producing trimethylamine. Detectable via urinary TMA test. This has a completely different chemical profile from PATM's toluene/mercaptan signature, and creates a distinct rotting fish odor, not a respiratory irritant.
M.C.S.
Multiple Chemical Sensitivity
In MCS, the environment triggers the patient. PATM is the inverse: the patient's emissions trigger the environment. The directionality of the trigger is completely opposite.
03. QUANTITATIVE PROOF
The first peer-reviewed study to objectively measure the skin gas profiles of PATM patients. Prof. Yoshika Sekine at Tokai University's Antioxidant Research Laboratory analyzed 20 PATM patients against 24 controls using GC/MS across 75 volatile compounds. Published in Scientific Reports (Nature).
Sekine Y, Oikawa D, Todaka M. Scientific Reports 13, 9471 (2023). DOI: 10.1038/s41598-023-36615-1
PRIMARY BIOMARKERS IDENTIFIED
TOLUENE
Petrochemical respiratory irritant. Found in paint thinner. Released through the skin via blood route.
ACETONE
Ketone emission marker linked to metabolic dysfunction.
HEXANAL
Oxidative stress biomarker. Reducible via anthocyanin supplementation (Willems 2022).
THE METABOLIC FAILURE RATIO
The study's researchers proposed that this Toluene-to-Benzaldehyde ratio disparity serves as a "vital sign" for a fundamental breakdown in hepatic metabolism. The working hypothesis is that when CYP450 enzymes in the liver fail to convert toluene to benzaldehyde, the unprocessed chemical accumulates in the blood and violently vents through the skin.
PATM mean ratio: 58.0
Control mean ratio: 0.076
04. OBSERVATIONAL PROOF
Scientific data only matters if it matches reality. I analyzed hours of raw community footage to see if the chemical data from Sekine manifested physically. It does. These are the three critical insights derived from field documentation.
EXHIBIT A1: ENVIRONMENTAL REPEATABILITY
CLINIC LOBBY RESPIRATORY IRRITATION
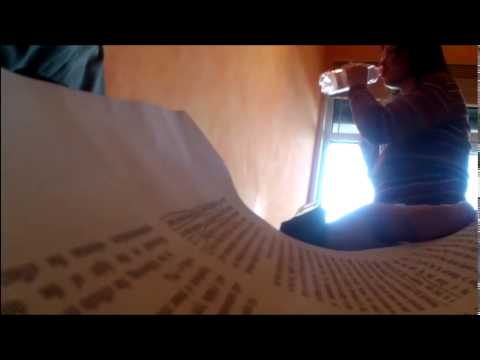
Candid camera footage inside a medical clinic lobby. The creator sits in a waiting room, and nearby patients and staff members begin rubbing their noses, coughing, and clearing their throats shortly after their arrival. To vent the room, staff open windows and doors, indicating a physical respiratory reaction to the air quality rather than psychological bias.
Clinic Lobby Observations
EXHIBIT A2: ENVIRONMENTAL REPEATABILITY
SYDNEY AIRPORT TRANSIT REACTIONS
Candid waist-level footage documenting pedestrian reactions as the creator walks through Sydney Airport terminals. As the creator approaches, passing travelers exhibit consecutive, sudden double-coughs and throat clearing. This indicates that reactions occur even in high-clearance, open-air transit hubs with strangers who have no prior knowledge of the sufferer.

Sydney Airport Transit Reactions
Waist-level candid footage disembarking a plane and walking through Sydney Airport waiting terminals. Note rapid-onset coughing and consecutive 'double-coughs' from passing travelers.
Reactions occur even in high-clearance, open-air transit hubs with strangers who have no prior knowledge of the sufferer.
EXHIBIT A3: ENVIRONMENTAL REPEATABILITY
PHD PRESENTATION AUDITORIUM REACTIONS
Audio-visual capture during a 44-minute PhD research presentation delivered by the creator. Colleagues and professors seated in the lecture hall are recorded frequently coughing, clearing throats, and showing physical discomfort. The persistence of reactions in an academic setting highlights the consistent nature of the chemical emissions across different environments.

PhD Presentation Auditorium Reactions
Floor-level compile of loud coughing incidents during my 44-minute PhD research presentation to a room of academic colleagues.
Colleagues and professors seated in the lecture hall are recorded frequently coughing, clearing throats, and showing physical discomfort.
EXHIBIT A4: ENVIRONMENTAL REPEATABILITY
RESTAURANT INDOOR AIR CONVECTIVE BLOWBACK
Hidden camera footage recorded inside a restaurant dining room. The camera captures a couple seated at an adjacent table directly downwind from the air conditioning unit. As air flows past the creator toward them, they begin coughing and sneezing, illustrating how air convection currents transport the volatile chemical cloud.

Restaurant Indoor Air Convective Blowback
Silent, sideways hidden camera recording inside a wood-panelled dining area. Captures physical reactions from a couple sitting in the path of the air conditioner blowback.
As air flows past the creator toward the couple, they begin coughing and sneezing, illustrating how air convection currents transport the volatile chemical cloud.
EXHIBIT A5: ENVIRONMENTAL REPEATABILITY
CLASSROOM RESPIRATORY CHORUS (AUDIO ONLY)
An audio-only recording captured during a class. Sufferer Victoria records the sounds of classmates repeatedly coughing, clearing their throats, and coughing in rapid succession. The screen is kept pitch black to protect student privacy and due to classroom policies.

Victoria's Pinned Comment (Classroom Audio Uploader)
Hi guys. I've gotten almost no reactions this past year. 1) Always eating on time never skipping meals. 2) Going to check for h pylori and treatment for it. 3) Quitting spicy, fried, acidic, citrus, etc any other food that hurts your stomach. Lots of green veggies. 4) Probiotics 5) Eating small meals instead of 3 full meals I ate 5 small meals. Please don't hesitate to contact me at ixxvictoriaixx@gmail.com
An audio-only recording captured during a class. Sufferer Victoria records the sounds of classmates repeatedly coughing, clearing their throats, and coughing in rapid succession. The screen is kept pitch black to protect student privacy.
EXHIBIT B: SYSTEMIC VS LOCALIZED
THE FAILED CURE
A crucial piece of testimony involves a PATM/TMAU sufferer who pursued medical treatment expecting a cure, only to find it failed entirely. This reinforces the functional model: targeted interventions that do not address the underlying systemic metabolic dysfunction -- the liver-gut axis and oxidative stress cascade -- are unlikely to resolve the condition.

Video Description Context & User Comments
"This video is more or less about how I thought I was supposed to be “cured” due to the cystic surgery I had, but unfortunately I was not, so I discuss setbacks and going back to work..." (Jun 8, 2021)
"...I do low and non fat it helps me with the burnt smell and now Bubbies fermented dill pickles I drink some of the juice and eat a pickle and it kind of keeps the burnt smell from being too strong and lasting a long time..."
"Unfortunately, there is no cure for TMAU its a genetic disorder. You can treat it with diet restrictions but no cure unless you have secondary TMAU (TMAU2) which is not genetic..."
EXHIBIT C: INDEPENDENT SYNTHESIS
THIRD-PARTY VALIDATION
Independent synthesis of PATM testimonies confirms the condition's catastrophic sociological impact. Within the Inufusa framework (explained below), this intense career destruction and social isolation is theorized to feed directly back into the oxidative stress cascade, potentially worsening the physical emissions as psychological stress increases.
Sufferer Testimonies & Community Notes
"7years and counting this PATM, isolation a lot. Hurt too muchhhhhhhhhhhhhh"
"I also have PATM and it's been thought that it's a problem with liver."
Suggests checking CaSR gene mutations, parathyroid hormone, Ca, P, Cl, K, Na, indicating a potential renal/kidney pathology.
CLINICAL FRAMEWORK 01
THE FUNCTIONAL MODEL
DR. YASUHIRO KONISHI -- Board-Certified Internist. Director, Konishi Integrative Medicine Internal Clinic, Osaka. Functional Medicine Specialist.
WHY HIS DATA MATTERS
Dr. Konishi is the only physician in the world who has publicly stated he has examined over 1,000 PATM patients. He is entirely unambiguous: "I am absolutely convinced this is not a delusion."
THE LIVER-GUT AXIS
- Uses skin gas testing as a diagnostic tool, not psychiatric evaluation.
- Identifies liver detoxification failure (Phase I / Phase II) as the central mechanical breakdown.
- When the liver cannot process chemical loads, the body defaults to exocrine venting (through the skin).
- Identifies gut dysbiosis as the root trigger disrupting the CYP450 enzyme function in the liver.

PATM: A Doctor Explains
サクッとわかる機能性医学 (Dr. Konishi)
Clinical Framework Context:
Dr. Konishi's Core Diagnosis: PATM is driven by severe gut microbiome imbalance (腸内環境の乱れ) combined with reduced systemic detoxification capacity (解毒・デトックス機能 of the liver). He emphasizes that it is a physical, metabolic skin gas condition, not a delusion.
CLINICAL FRAMEWORK 02
THE OXIDATIVE STRESS MODEL
DR. HARUHIKO INUFUSA -- MD/PhD. Specially Appointed Professor, Antioxidant Research Division, Gifu University.
Dr. Inufusa expands on why the liver fails. He identifies oxidative stress as the primary destroyer of CYP450 enzymes, locking the sufferer into a catastrophic biochemical feedback loop. This is the detailed breakdown of the Inufusa Cascade.
THE TRIGGER (Psychological & Environmental)
Biology: Severe chronic stress (trauma from bystander reactions, isolation) activates the HPA axis. The body floods with cortisol and adrenaline, locking into a continuous sympathetic "fight-or-flight" state.
THE ROS EXPLOSION (Oxidative Stress)
Biology: Prolonged stress forces mitochondria to overwork. The system begins overproducing Reactive Oxygen Species (ROS)—highly unstable molecules. Natural antioxidant reserves (Glutathione) are rapidly depleted, inducing severe oxidative stress.
THE HEPATIC BOTTLENECK (CYP450 Impairment)
Biology: This is the critical failure point. Cytochrome P450 (CYP450) liver enzymes are responsible for breaking down foreign chemicals. The excessive ROS molecules violently damage these enzymes. The liver's chemical processing plant shuts down.
THE CHEMICAL BACKLOG (Toluene Accumulation)
Biology: Everyday chemicals from air, food, and gut bacteria are absorbed but cannot be processed. Instead of converting Toluene into harmless Benzaldehyde for urination, unmetabolized VOCs build up heavily in the bloodstream.
THE ALTERNATIVE VENT (Skin Gas Emission)
Biology: Toluene and Hexanal are highly volatile. As saturated blood circulates through the dermis, these chemicals off-gas through the pores and breath, joining the body's natural microbial cloud.
THE BYSTANDER REACTION
Biology: The emitted VOCs are industrial respiratory irritants. When inhaled by a bystander within 2 meters, they chemically aggravate mucous membranes. The bystander involuntarily sneezes, coughs, or rubs their eyes (chemical irritation, not IgE allergy).
THE VICIOUS FEEDBACK LOOP
Biology: The PATM sufferer observes the bystander coughing. The sufferer instantly experiences a spike of intense psychological distress and shame. This instantly triggers Stage 01, generating more ROS, further destroying CYP450 enzymes, and making emissions stronger.

ANTIOXIDANT PROTOCOL
Dr. Inufusa developed Twendee X, a Grade A certified antioxidant supplement containing CoQ10, vitamins, and amino acids. While he has clear commercial interest in this product, the oxidative stress cascade science underpinning it is mechanistically sound.
Dr. Inufusa's Dietary Protocol
"Limit carbohydrates (糖質制限), eat dark-colored vegetables and fruits, avoid infectious diseases, alcohol, and smoking, and supplement with active antioxidants to suppress ROS."
Sufferer Testimonies & Clinical Notes
"I have been suffering from PATM for 20 years. The chemical skin gas causes self-damage (throat clogging, nose, and eye irritation in the sufferer themselves), which worsens significantly with psychological sweating."
Reports PATM symptoms starting suddenly after receiving a vaccination (correlating to sudden immune/metabolic shifts), experiencing others coughing, sneezing, and clearing throats in their presence.
"I also feel a strong discomfort/clogging in my throat (喉の違和感) when in public. It is a relief to know this physical symptom is a recognized aspect of PATM self-damage."
05. THEORIES OF CAUSATION
Why does the metabolic clearance system fail in the first place? Based on patient biochemistry, clinical data, and toxicology reports, the community has synthesized five primary root causes that trigger liver-gut dysfunction.
ONSET HYPOTHESES: THE TRIGGER EVENTS
How does the condition actually start? Below are the four primary clinical-grade hypotheses explaining the sudden or progressive onset of P.A.T.M. in sufferers, detailing the initial breakdown of metabolic and mucosal barriers.
Microbiome Decimation
Aggressive antibiotic courses wipe out protective gut flora, destroying mucosal barriers and leading to Candida or Rhodotorula colonization. The resulting massive gut endotoxin dump permanently overwhelms hepatic portal filtration.

Mold & Mycotoxin Saturation
Inhaling high concentrations of mycotoxins from black mold depletes cellular glutathione levels and damages mitochondrial membranes in hepatic tissue, causing systemic metabolic clearance failure.

Heavy Metal Saturation
Slow bioaccumulation of mercury, lead, or cadmium binds to sulfhydryl groups in glutathione-synthesizing enzymes. This halts liver detoxification and triggers oxidative damage across hepatocyte membranes.
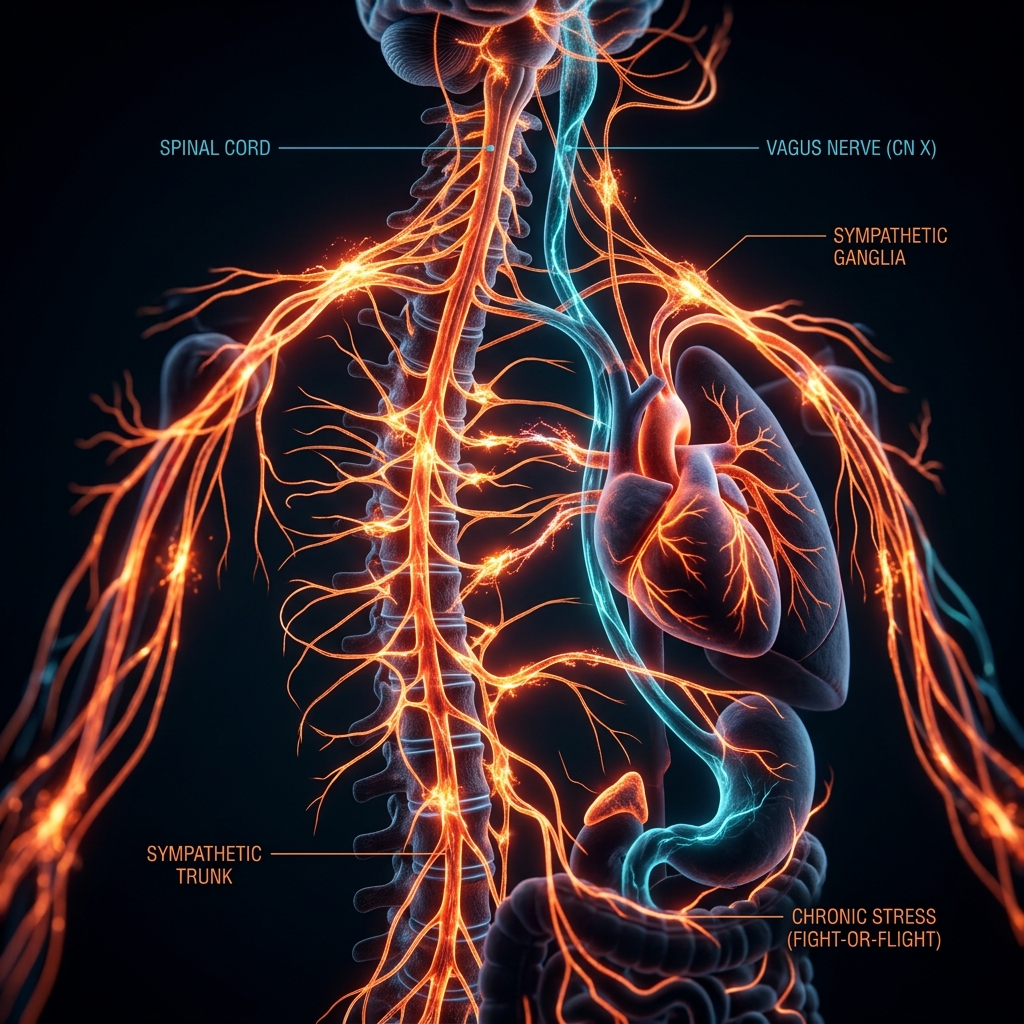
Autonomic Collapse
Severe neuro-autonomic stress locks the patient in sympathetic dominance, causing vasoconstriction that reduces hepatic blood flow by up to 40%. The resulting hypoxia halts enzyme synthesis and bile flow.
06. TREATMENT HIERARCHY
No treatments are clinically approved for PATM. Based on the mechanical breakdown outlined above (Liver Failure + Oxidative Stress), this is the prioritized intervention hierarchy derived from the data.
LIVER DETOX / CYP450 SUPPORT
Reactivate Phase I and Phase II detoxification to process the chemical backlog. Reduce external chemical burden.
KONISHI PROTOCOLOXIDATIVE STRESS REDUCTION (ROS)
Break the feedback loop. High-potency antioxidant supplementation (CoQ10, NAC, Anthocyanins) to protect remaining CYP450 enzymes from free radical damage.
INUFUSA PROTOCOLGUT MICROBIOME REPAIR
Address intestinal dysbiosis to stop the gut-liver axis from continuously triggering systemic inflammation.
FUNCTIONAL MEDICINELIFESTYLE MODERATION
Total elimination of alcohol (competes for CYP450) and smoking (increases skin toluene). Dietary shift to natural antioxidants (dark vegetables).
METABOLIC CONTROLPSYCHOLOGICAL INTERVENTION
You cannot stop the ROS explosion without stopping the psychological stress response. Managing the trauma of bystander reactions is biologically essential to curing the condition.
CRITICAL PATHWAY07. BIOPHYSIOLOGICAL PATHWAY ALIGNMENT
Community recovery testimonies consistently converge on gastrointestinal, dietary, and environmental protocols. This section maps these core gastrointestinal, dietary, and environmental interventions, alongside environmental mold and Rhodotorula yeast triggers, to the biochemical pathways identified by Prof. Sekine.
1. CYP2E1, FMO3, & GLUTATHIONE DYNAMICS
Dietary Pacing & Genotype Screening: Small meals & FMO3 assessment
Fasting hyper-induces Cytochrome P450 CYP2E1 while depleting liver glutathione (GSH). Concurrently, genetic variants or overload of the Flavin-containing monooxygenase 3 (FMO3) enzyme (associated with secondary TMAU/TMAU2) impair the oxidation of volatile nitrogen/amine compounds. Spanish MEBO Research protocols emphasize mapping FMO3 polymorphisms alongside renal clearance ratios (measuring urinary sodium/potassium imbalances). Spreading food into 5 small meals preserves glycogen and glutathione, buffering amine and VOC surges.
2. GASTRIC UREASE AMMONIA LOAD
Gastric Screening: H. pylori detection & eradication
H. pylori releases massive quantities of urease to hydrolyze gastric urea into volatile ammonia (NH3) and carbon dioxide (CO2). Gastric mucosal inflammation allows these volatile gases to enter portal circulation. In individuals with sluggish liver clearance, this excess gas load bypasses filtration and vents via the lungs and skin. Eradication removes this major source of systemic volatile nitrogen compounds.
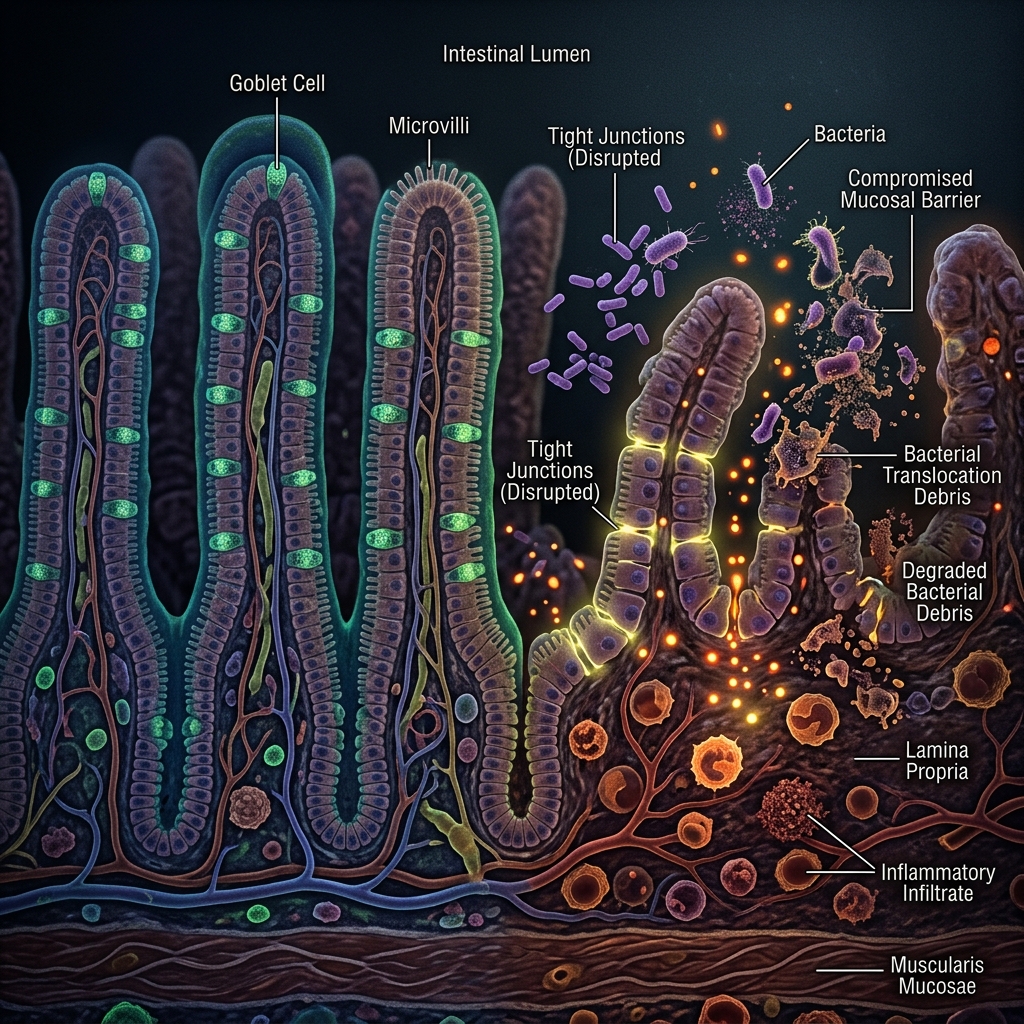
3. MUCOSAL BARRIER INTEGRITY & BINDERS
Barrier Protection: Gut integrity, green vegetables, & probiotics
Inflammatory foods damage tight junctions ("leaky gut"), allowing volatile microbial metabolites like organosulfurs (e.g., methyl mercaptan) to directly cross into portal blood. Probiotics displace anaerobic sulfur-reducing bacteria, while green vegetables provide folate and magnesium to support methylation. Taking carbon-based binders (activated charcoal) intercepts and adsorbs these compounds in the gut lumen, preventing systemic absorption.
4. ENVIRONMENTAL MOLD & MYCOTOXIN OVERLOAD
Environmental Control: Mold Binders, TCM Damp-Heat, & Antifungals
Indoor water damage triggers severe hepatic and mitochondrial toxicity. This state maps closely to the TCM Damp-Heat (湿熱) paradigm, representing high humidity, fungal/mold toxin overload, and congested fluid transport (脾胃虚弱). Chinese clinical forums suggest dispelling Damp-Heat via traditional herbal decoctions (e.g., Ganlu Xiaodu Dan) to resolve tissue toxins, alongside physical Qigong (Baduanjin) to normalize autonomic perfusion and enhance mucosal defenses against environmental molds and colonizing yeasts.
RESOURCES
COMMUNITIES
r/PATM -- Reddit peer support
MEBO Research -- Spanish/English testing hub
Baidu PATM Tieba (百度PATM吧) -- Chinese patient portal
Zhihu PATM Discussion -- TCM & gut logs
MedHelp PATM Forum -- Historical source
KEY PAPERS
Sekine et al. 2023 -- Scientific Reports 13, 9471
Meadow et al. 2015 -- "Personal microbial cloud" PeerJ 3:e1258
Willems et al. 2022 -- Anthocyanins reduce hexanal
CLINICS
Konishi Clinic -- Osaka (Integrative)
Antioxidant Res. -- Gifu (Dr. Inufusa)
Kunitachi Clinic -- Tokyo (Integrative)
Candid footage showing staff and patients in a clinic waiting room. Shortly after sitting down, nearby people start coughing, clearing their throats, and rubbing their noses.
To vent the room, staff open windows and doors, proving a physical respiratory response to the air quality rather than psychological bias.